
Tendon Neuroplastic Training
Written by Rucha Gadgil, Janhavi Manjrekar
Graphics by Riddhi Gandhi
Visual Media by Chinmayee Patil
Imagine yourself with an athlete with Achilles tendinopathy. You are incorporating strength training and other techniques but with a small new additional technique. This new addition will help in bilateral cortical activation and is easy to incorporate into your rehab plan. Go ahead and read about this new skill set that can be added and applied to your rehab protocol today!
Why are Tendons a challenge to treat?
- The slow and long recovery period.(Whopping 89% of patients taking up to one year to recover.)
- High chances of re-aggravation of symptoms.
- Several patients remain unresponsive to the traditional treatment.
- The recurrence rate is usually high even after the treatment. (Research shows that 10% of tendinopathy cases continue to experience long-term pain and disability.)
So, this technique can prove to be a welcome milestone in the treatment of chronic tendinopathies.
What are Tendons?
Tendons are a part of the muscle-tendon unit, which works together with the bone and muscle to absorb the load. It behaves like a complex spring to manage the load it is exposed to, which is nothing but its load capacity. For example, a recent study states that tendons are subject to mechanical loading during running, almost like 6-7 times body weight.
Tendinopathies what are you?
These injuries are the collagen breakdown in the tendons, which usually take weeks to a few months to heal.
Pathologically speaking, these injured tendons show an increased tenocyte cell size and number, disorganized collagen, increased proteoglycan and water content, neovascularization
What happens beyond the tendons in Tendinopathy?
Evidence has also demonstrated alterations to the motor cortex in patients with this condition, along with measurable changes in corticospinal excitability and short-interval cortical inhibition.
There is evidence showing increased cortical inhibition to be linked with phasic nociceptive stimuli. There is also greater corticospinal excitability (CSE) registered than in normal tendons, altering the balance of excitability and inhibition of motor control compared with the healthy population.
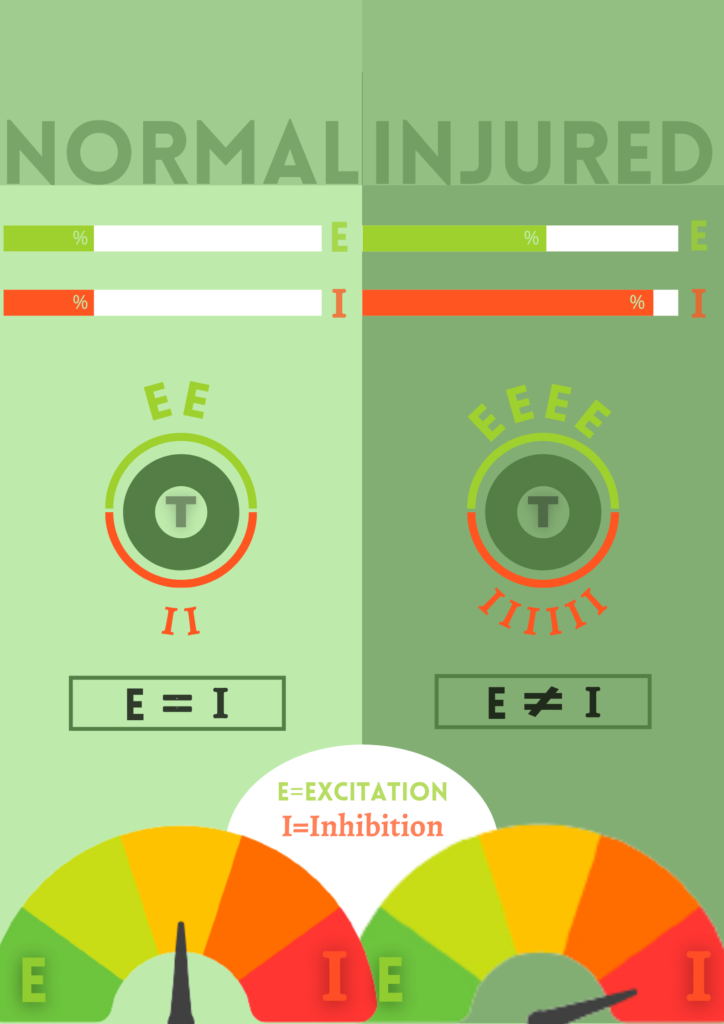
The motor control strategy can be compared to a novice driver controlling the speed of their car with one foot on the brake and one on the accelerator, i.e., the car breaks down a great no. of times.
There are reports associating adaptations in the unaffected side after tendinopathies, i.e., alterations in the motor control on the normal side. For, e.g., a study by Heales et al. reported that the asymptomatic side was weaker in upper limb tendinopathy when compared with a control group. The science behind this has been connected to alterations of the corticospinal pathways following the injury, mainly increased interhemispheric inhibition similar to that seen in stroke.
The variety of treatment paradigms that exist may show an improvement in restoring the muscle and tendon properties.
What is Missing?
- The high recurrence rates and the adaptations seen on the unaffected side have also been linked to the self-paced (self-selecting the intensity of the exercise) programs being practiced.
- The standard treatment modules also do not adequately address the differences in the cortical firing rates seen in tendinopathies.
What exactly is tendon neuroplastic training?
Tendon neuroplastic training improves motor control at its core.
Cortical inhibition has been reported to be a feature of Tendinopathy, according to Rio et al. (2015), which means that the area of the brain that controls the muscle, which is your motor cortex shows slight alterations. The balance between excitation and inhibition is affected in tendinopathy patients.
TNT includes external pacing to the tendon rehabilitation exercises using a metronome/visual aid to improve motor control and help restore this balance. These metronomes give auditory/visual cues that match the isotonic/isometric exercise regimen and strength training.

There is a potential to reduce the pain in tendinopathy patients by altering the cortical pathways.
Studies show the use of external pacing, with-
1. A metronome
The individual would contract concentrically and eccentrically to the sound of the metronome and complete these phases as prescribed.
2. A visual cue
Matching the contraction phase’s pace with a visual cue causes an increase in excitability in both skills visuomotor tracking and short-term resistance training. It improves muscle activation and cortical/subcortical firing), i.e., activates the motor cortex and its pathways.
This addition of neuroplastic training is purely practical. Heavy, slow resistance training, which is meant to be done “Slowly.” A contraction of 3 seconds for the concentric component, followed by 3 seconds of an eccentric component with eight repetitions (48 s set×4) with a 2 min rest to the beats of a metronome, is successful in the tendon rehab world. However, the exact frequency, intensity, duration, and type of exercise are still up for debate.
Noteworthy Considerations
When treating a tendinopathy case, it is also essential to account for the load capacity of local tissues and the capacity of the entire kinetic chain. For example, for a runner with Achilles’ Tendinopathy, we should target:
- Tissues at the local level at the site of injury
- The entire kinetic chain (Depending upon what is relevant to the demand of sport/daily life)
Factors to make a note of before planning the Rehabilitation Protocol-
- Non-Musculoskeletal Intrinsic profile (Diet, age, BMI, Medication, Metabolic factors, hormonal change.)
- Brain and CNS (Where the TNT plays a role)
- Psychosocial factors (Stress, mood, fear, thoughts, beliefs, rehab behaviors, and motivation)
Take away: Tendon neuroplastic training is an idea of doing strength-based loading as an essential stimulus for the tendon and muscle, with strategies known to optimize neuroplasticity of the motor cortex and drive to the muscle. It improves motor control by reducing cortical inhibition and normalizing excitability. We must adapt and progress as newer mechanisms behind injuries are found as more research is needed to test this concept; TNT provides a welcome change in tendon rehabilitation.
References
- Coombes BK, Bisset L, Vicenzino B. A new integrative model of lateral epicondylalgia.Br J Sports Med. 2009 Apr; 43(4):252-8.
- Bhabra G, Wang A, Ebert JR, Edwards P, Zheng M, Zheng MH . Lateral Elbow Tendinopathy: Development of a Pathophysiology-Based Treatment Algorithm.Orthop J Sports Med. 2016 Nov; 4(11):2325967116670635.
- Welsh P. Tendon neuroplastic training for lateral elbow tendinopathy: 2 case reports. J Can Chiropr Assoc. 2018 Aug;62(2):98-104. PMID: 30305765; PMCID: PMC6173218.
- Rio E, et al. Br J Sports Med 2016;50:209–215. doi:10.1136/bjsports-2015-095215
- M. Leung, T. Rantalainen, W.-P. Teo, D. Kidgell.Motor cortex excitability is not differentially modulated following skill and strength training. Neuroscience,2015. 305:99-108, ISSN 0306-4522
Contributors
RUCHA GADGIL
Research & Content Writing Team

JANHAVI MANJREKAR
Research & Content Writing Team
CHINMAYEE PATIL
Multimedia Team

RIDDHI GANDHI
Art Director